
As my ‘love affair’ with New Zealand Aotearoa’s public health system grew over many years I learnt to pick up on a few soundbites that aptly summarised it. One was that if something made good clinical sense it would also make good financial sense.
With the arrival of the coronavirus pandemic (Covid-19) in March 2020 Prime Minister Jacinda Ardern’s government took the advice of experts which, in effect, meant adopting the principle that what made good public health sense also made good economic sense.
Good public health and economic sense
This led to New Zealand’s successful elimination (zero tolerance) strategy towards community transmission. The outcome was both one of the lowest Covid-19 mortality rates in the world and the best performing economy in the Organisation of Economic Cooperation and Development.
Strong active political leadership continued when the Delta variant of Covid-19 hit our shores in July last year and right up towards the end of September. Then the Government unfortunately accepted overconfident advice from the Ministry of Health to lower Auckland’s alert level from four to three (a lesser form of lockdown). Unsurprisingly to many, the declining hospitalisation rate reversed upwards.
The Government can be excused for accepting wrong advice. But it then panicked and made things worse by a confusing abandoning of the elimination strategy in Auckland (thereby increasing the length of total lockdown). Until this time the Government had been affirming correctly that it was ‘following the science’ (ie, the evidence).
But, while this expertise was largely within the health system, most of this was outside the Health Ministry. The public strongly supported the Ardern government’s Covid response because it was seen to be ‘following the science’.
However, this point of departure in late September, not helped by a muddled media presentation, led to public confidence slowly but steadily diminishing. It also marked the turning point for declining poll performances.
The widening gap continued with decisions like replacing the more familiar alert system with the confusing traffic lights system. Now, on 21 March, it took a quantum leap, with Ardern’s announcement of the removal of most restrictions designed to protect against the Omicron variant of Covid-19.
Significantly, according to reported comments from Director-General of Health Dr Ashley Bloomfield, he and his ministry were not asked to provide advice on this issue. Epidemiologists and other experts were even further out of the decision-making loop.
Moving towards laissez-faire
21 March marks the biggest step towards a laissez-faire pandemic response that has prevailed in many developed economies including in Europe and the United Kingdom. Obviously a French expression, laissez-faire is a policy of minimum governmental interference.

Another description is abdication of responsibility while allowing those holding economic power to continuing exercising their power. While usually associated with the economy, laissez-faire is also the opposite of public health measures in pandemic responses.
Not all restrictions are removed – mask wearing and vaccine mandates for the health sector and aged care remain. Further, the removal of restrictions for outdoor activities generally make sense.
But, overall it represents a significant shift towards laissez-faire and closer to the position of the high-risk approach of the National Party (to a lesser extent ACT’s).
Immediate reactions
Newsroom investigative journalist Marc Daalder wrote a skeptical article three days later (24 March): Sceptical analysis of Government’s announcement of removal of restrictions.
Two days later Auckland University microbiologist Associate Professor Siouxsie Wiles had an article published by The Spinoff: Two years since first lockdown.
She provides a good positive outline of the Government’s overall response to Covid-19. This includes a dramatic graph of deaths per million people which shows for much of the time how well Aotearoa compares with the United States and the United Kingdom.
But, alarmingly the graph shows a turn for the worse with these comparative Omicron mortality rates noticeably narrowing.
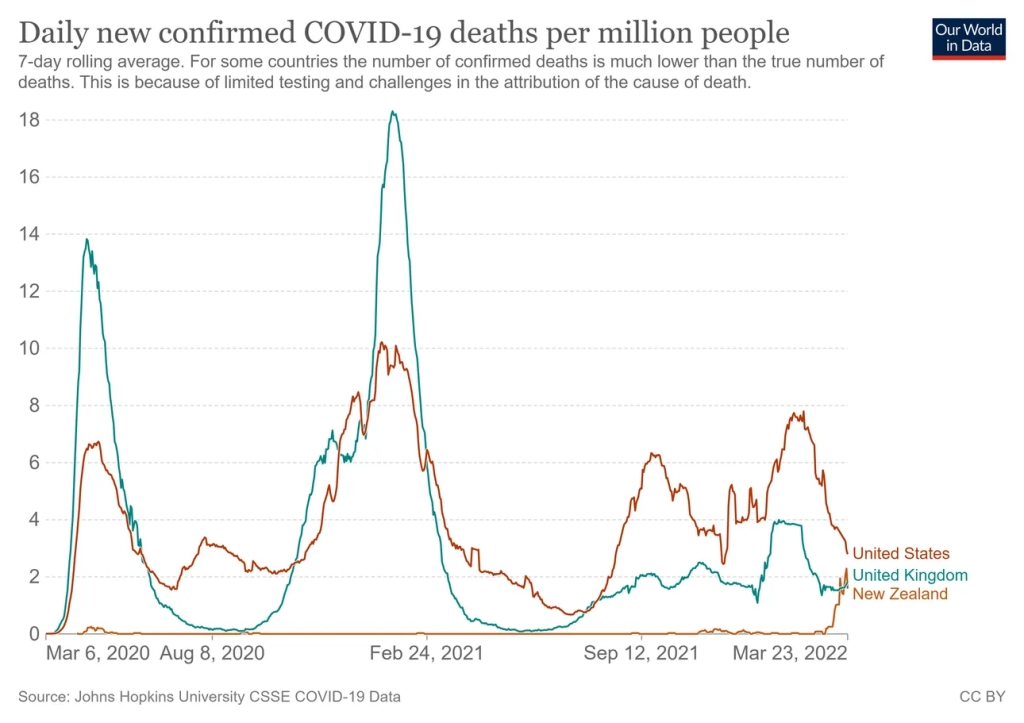
Dr Wiles warns against abandoning all protections when Omicron cases start to come down because a conceivable outcome, based on recent overseas experience, is that they start to rise again (ie new waves of infections leading again to rising hospitalisations and deaths).

Longer-term effects on children
The University of Otago publishes an excellent blog called Public Health Expert. Written by public health specialists and other relevant experts it is a must read for those who want to know more about population health including pandemic responses.
It is unfortunate for New Zealanders that relevant government ministers, including the Prime Minister either did not consider or disregarded its 9 March posting on children of longer-term (post-acute effects) of Covid-19 in children and ‘long Covid’: Greater efforts needed to protect children from infection.
The authors identify three main groups of post-acute effects on children:
- Multisystem inflammatory syndrome in children, a severe syndrome that occurs from about two weeks after the initial illness. Its peaks typically occur 2-5 weeks after peaks in acute infections.
- Longer-term effects grouped under an umbrella term (‘long Covid’) characterised by symptoms and pathology that persist beyond the acute episode. Almost any organ system can be involved. Common features in children are fatigue, sleep disturbances, headache, poor concentration, and loss of smell or taste.
- Chronic conditions that were known prior to the pandemic and are now being seen with new onset triggered by Covid-19 infection such as damage to heart, lungs, and brain.
For good reason the authors recommend a precautionary approach be taken in order to minimise widespread Covid-19 infection among children. A number of specific measures are proposed, including a lower threshold for closing schools and early childhood facilities with greater support for temporary home learning when community transmission is high.
Radio New Zealand has done an informative interview on the risks of ‘long Covid’ in Nine to Noon in an interview with cellular immunologist Dr Anna Brooks: Warnings about long Covid.
Experts’ advice on what restrictions should remain
Another Public Health Expert published on the same day as the Prime Minister’s announcement (21 March) focusses on what restrictions should remain: Control measures still need to be maintained.
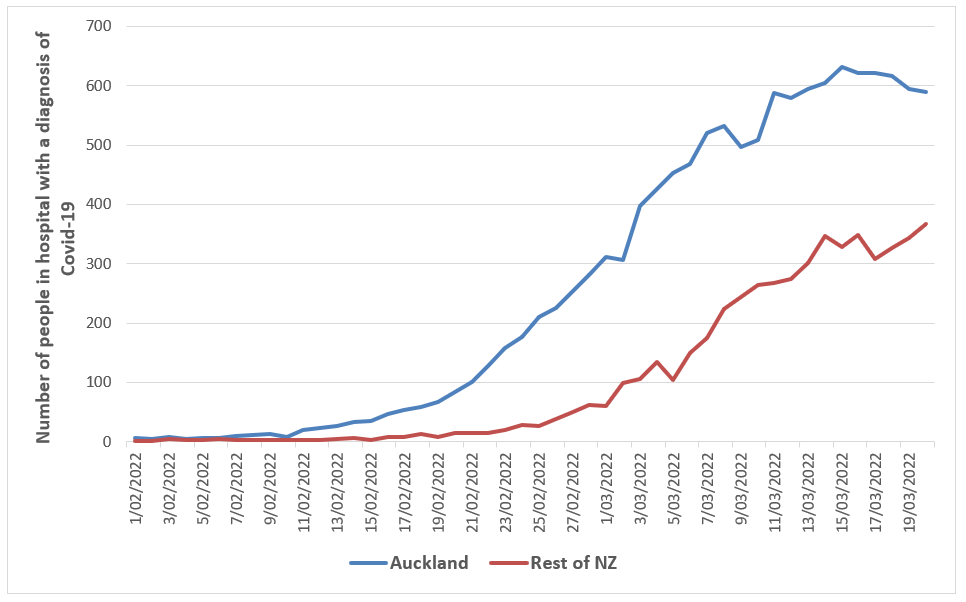
Its authors look at hospitalisations as a more valid indicator of the Omicron peak than daily case numbers. While Auckland’s hospitalisations likely peaked on 15 March we are still waiting for much of the rest of the country to do so. The peaks for patients in intensive care and daily deaths may also be yet to come.
A helpful graph is provided comparing hospitalisation in Auckland with the rest of New Zealand (1 February to 20 March).
With the necessary shift from elimination to mitigation of Omicron transmission (due to its extraordinarily high infection spread) and with the Government’s drift towards laissez-faire, the authors advise caution.
Even though the pandemic wave may be starting to decline, there are still tens of thousands of people being infected every day. Consistent with Siouxsie Wiles, these experts note the international pattern of declining infection numbers followed by increasing numbers under a new wave.
The only thing certain about the medium to long-term trajectory is high uncertainty. Consequently they recommend protective control measures which include the following:
- Raise levels of third dose coverage Covid-19 vaccination coverage. Rather than use the confusing term ‘booster’ (which implies a lower level of importance), specifically require that to be fully vaccinated against Omicron three doses are required. The two-dose requirement was sufficient for the Delta variant but is insufficient for the much more transmissible Omicron.
- Given the serious risks, including ‘long Covid, raise the levels of vaccination coverage among eligible children.
- Continue but upgrade the vaccine pass to three doses. The vaccine pass is important both for the safety of the public from virus transmission and incentivising the third (‘booster’) dose. The current vaccine pass was designed for the Delta variant. If Omicron had not occurred it would now be redundant. But Omicron has come.
- Keep mandatory mask use in key indoor settings, particularly: public transport (including aircraft), all healthcare settings, and in aged-residential care settings. This will also help with preventing other respiratory infections in the coming winter months. To date, the Government appears to still be committed to this.
- Continue making ventilation improvements for indoor environments, notably schools and workplaces.
- Continue to promote people staying at home when unwell and offer support to those who are isolating at home when they test positive for Covid-19.
- Maintain essential border biosecurity measures against Covid-19 by requiring arrivals (non-New Zealanders at least) to be fully vaccinated (ie, three doses) reinforced by a well organised system of testing
Summarising it all
It is important to appreciate that while Covid-19 is a respiratory virus, it is not just a respiratory virus. It does not just effect the respiratory system; somewhere between several and most other organs are at risk of damage.
Until late September 2021 New Zealand’s pandemic response was based on a public health approach which both protected the public’s health and served its economy well. It could genuinely be described as world-leading.
Since then it has gradually evolved towards laissez-faire with the Government’s 21 March announcement marking an acceleration of this evolution. From world-leading we have evolved to world-following.
Claims that we still have among the strongest restrictions in the world (masks and limited mandates) are overstatements given that Aotearoa was one of the last countries that Omicron hit and how we are trending.
To the extent that children, their families and other New Zealanders suffer more or die as a consequence of this evolving laissez-faire approach, responsibility will rest squarely and fairly with the Government. Bending to external political and other pressure does not mitigate this responsibility.
Let us not forget that today (29 March) we had 34 deaths; not only our highest daily number but also higher than the total deaths from the start of the pandemic in March 2020 until the impact of Delta in August 2022.
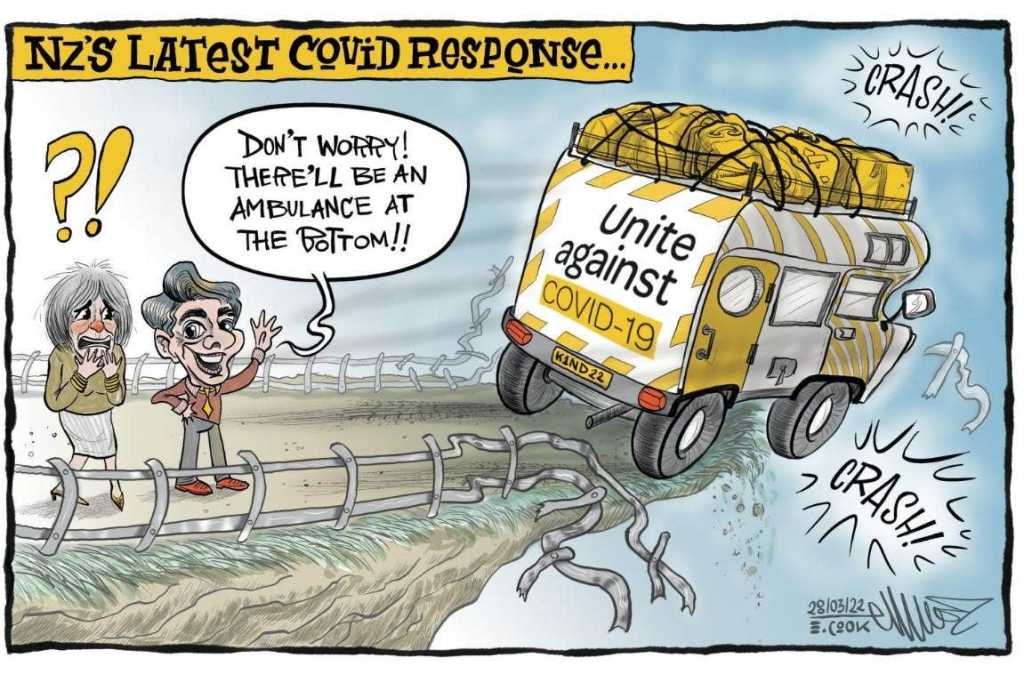
Perhaps trumping both Marc Daalder and Siouxsie Wiles, the best summation of the Prime Minister’s 21 March announcement, is cartoonist Emma Cook five days later.
If I ruled the pandemic response
Responsibility for the pandemic response, including any abdication, rests with the government of the day. I don’t determine the pandemic response and, unfortunately, neither does Welsh comedian and opera singer Harry Secombe. Advice from Harry Secombe.
But, if I did rule the pandemic response, this is what I would do while Omicron continues to have a significant presence:
- Shift back from laissez-faire to explicitly making public health the central focus of the response. Given the current severity of workforce shortages throughout the economy, the more the health of the public is protected the more economic performance can be improved. It is too early for the economic analysis to be done, but the economic impact of Omicron may well be more severe than official lockdowns.
- Require three vaccine doses before a person can be categorised as fully vaccinated.
- Require vaccine passes (fully vaccinated for Omicron) for keey indoor facilities including cafes.
- Only vaccinated children allowed to attend school (online home support for unvaccinated children). With already more than 200,000 children staying home from school every day this month during the Omicron surge, this is hardly going to more disruptive for children and teachers. Unvaccinated children disproportionately spread the virus. Being infected by Omicron also delays access to vaccination for children. This also impedes access to spread to themselves and others.
- Vaccine mandates for schools should be reintroduced particularly for those required to interact with children and other staff.
- Provide effective respiratory masks free to all as recommended by Associate Professor Collin Tukuitonga (University of Auckland).
The Government needs to adopt a strategic pandemic response that is rooted in public health. This makes good sense for the health and well-being of the public; it makes good sense for the economy; and it is likely to make good electoral sense as well.
Ian Powell was Executive Director of the Association of Salaried Medical Specialists, the professional union representing senior doctors and dentists in New Zealand, for over 30 years, until December 2019. He is now a health systems, labour market, and political commentator living in the small river estuary community of Otaihanga (the place by the tide). First published at Otaihanga Second Opinion



A very long OP but a couple of points.
Yesterday there were 34 deaths reported from the past 10 days. Confusing but assumed it’s prior to those who subsequently tested positive for Covid but this was not known until after death.
Caroline MacElnay stated yesterday they had Covid at the time of death, but the linkage otherwise suggests it was not the cause of their death, it’s just that they had it. “Evidence to date suggests some of these deaths will not be caused by Covid 19”. It could well be most!
And I will assume we have been all along attributing anyone who dies and happens to have Covid as Covid been the reason for their death. The most infamous reporting of a Covid death was the man shot to death in motel driveway late last year. The stats chalk him up as a victim of Covid, not that he was murdered, which he so obviously was. He probably didn’t even know he had it!
This fear that radiates out of the MOH from this misreporting, if taken at face value, is outrageous. It has closed a normal functioning society down as people are convinced the risk is too high. The costs of that are building.
Which brings me to the second point. Auckland especially is over it. We were shut off from the rest of the country for months, unable to leave NZ for fear of being locked out based on this flawed numbers game we have so far trusted. For the rest of NZ these lockdowns barely changed anything, great, no skin off your nose, for Auckland, the effect was far worse. World leading it was not.
Science can say whatever it likes but rigged stats undermine it’s credibility. And when the people no longer want to hide under their beds, governments must let go. We have all seen Omicron or most of us have. It’s worse than an ordinary cold but not much more on the vast vast majority of cases.
Our government hasn’t panicked, it just got real! It had to!
Well said
Exactly right X Ray!
Deaths WITH Covid but not necessarily OF Covid. Take a look at the age distribution of pandemic deaths in Australia (which maintains full transparency, unlike here):
https://www.statista.com/statistics/1245896/australia-number-of-coronavirus-deaths-by-age-group-and-gender/
The majority of deaths are among those older than the average lifespan. According to Aussie media reports, large numbers of these deaths were in dementia wards and hospices. Was this really worth ruining the educational chances of kids coming from the lower socio-economic homes? Where there is no laptop for Zoom classes or it is shared among a family of ten? The ugly consequences of the lockdowns will echo for many years.
This is an interesting opinion from a layman..
He has an MA in History and Political Science from the University of Canterbury and a Diploma of Industrial Relations from Victoria University of Wellington.
Presumably if x% of the population has a covid infection, then x% of peopled dyeing on any particular day will also have covid. likewise people in hospital will follow the same proportionality; just as if the percentage of the population with red hair and freckles is y% it can be assumed that y% of people in hospital on any day will have red hair and freckles. The potential difference being that every death and every hospitalisation is tested for covid whereas only some of the wider population will be tested, or their positive test result recorded.
We are in the midst of a pandemic of deception.
D J S
Brother, you going down the Tory dirty politics rabbit hole, some of your mathematics is suspect. !6% of population are Maori, 12% pacifica, but Covid deaths are near 18 and 19% for Maori and Pacifica. You might be a fit young pakeha and not worried about infecting elderly or sick whanau but I’m Maori over 70 years and immunocompromised so I really am fearful of covid and my health especially as Aotearoa is going through high case numbers and deaths at this moment. I always wear a mask, record QR code, keep apart from crowds and I do my own research but I’ll still listen to advice from Jacinda and the scientists not conspirators, I reckoners, and antivaxxer lunatics.
I do hope you come through unscathed Nikorima; I am also over 70. but fortunately in good health.
My point was that at this stage covid as omicron does nt seem to be any more of a danger to us than many common viruses that have plagued humanity for ever. At the beginning we did not know. No one did and I suspect that the first strain that emerged was much more dangerous than quite early mutations and it became more benign more quickly than anyone has realised even well before omicron. But the distortion of reporting the effects from all over the world has been a scandal .
Cheers D J S
OK, I’m 73, tested positive 4 weeks ago, minor symptoms. Friends have also tested positive, we’ve all done the right thing and stayed home.
People I interact with stay at home if they test positive but mostly we don’t care.
Well said.
Not to mention so much of the wisdom of the experts has proven to be fanciful fiction.
There is no evidence to suggest “Unvaccinated children disproportionately spread the virus”. He jsut wishes it was the case so he could justify forcing the jab on any kid who wants to be at school.
Just one example of the whole mantra “following the evidence” being a politcal canard. The evidence doesn’t go anywhere. What is or is not evidence and what it means is a human construct, with biases and political and economic interests. The BMJ recently published an article outlying what we all already knew but “PHS experts” like to pretend is not the case. The whole global health system is hopelessly captured and corrupt.
Hence This “expert” apparently forgetting the first rule of Public health. “Do No Harm”. And that has been smashed by the self-interested industrial health complex. Intervention is a HUGE responsibility. Treating us like tech to be upgraded, the new philosophy is “Move fast and Break THings”. We are thick in the realm of massive unintended consequences and they are hoping we keep listening to them, and don’t notice.
I was going to say you missed the most important one of all – KEEP PEDALLING THE FEAR!
But actually the whole article is about that, well done.
Option B is we do what the rest of the world is doing, accept it’s endemic, accept it will be here for years and accept we need to learn to live with it, without restrictions.
You can live with it ma but where is pa did covid get him to
Well CIP, pa was my grandpa, he died about 10 years ago, I am fairly confident covid didn’t get him… He was 94 though so not a bad innings I think you’ll agree?
Fortunately covid hasn’t yet got my Ma and Pa.
Which is good as they’re coming here on Friday with a freezer full of venison that Pa has shot and for which I’ll swap him some good home kill beef for out of our freezer.
This MA is not a ma though, just my initials but I do appreciate you concern for pa.
Your list of recommendations at the end is not based on scientific evidence at all. It is based on your own fear issues regarding COVID-19.
Because this is the problem in this whole pandemic response, at a worldwide scale: we lack good evidence. Good evidence is meta-analyses and randomized controlled trials, not the scientific buddies of Labour meeting at the corner of the table. Experts’ opinion is the LEAST good form of evidence, by far, experts have been wrong all the time in medicine history, when they are not riddled with conflicts of interest, to start with.
Do we have good (I insist on good) evidence that vaccinating children does actually anything to protect them or protect the people around them? No.
Do we have good evidence that boosters are useful and safe against Omicron vs. the standard double dose? Neither. For the safety aspect, I was recently happy to finally hear from the IMAC head himself that yes, Pfizer 2nd and booster doses cause more myocarditis in young males than COVID-19 itself, as it was shown in the Nature study when you analyze their figures in details.
The only solid piece of public health advice at the moment comes from WHO saying basically that rich countries like us should stop worrying so much about vaccinating kids and getting boosters done and instead should shift towards more efforts to protect less developed countries, as these ones are the perfect incubator for new variants to emerge.
Why do you want to keep unvaccinated kids from school? This does not make any sense from a public health perspective. We know this vaccine is not good at preventing transmission (around 50% reduction only the first weeks before this effect vanishes) and we actually lack solid data on it protecting kids from hospitalizations (but likely to be the case). On the contrary, we know that diverting kids from their usual place of socialization and learning can have a huge impact on their development. For a lot of poor kids, there is no education at home for them and no incentives to attend online classes. Sometimes even no safety. School is a reassuring haven for them. The teacher remains a role model for a lot of children. Why would you deprive them from all of these positive aspects of schooling in the name of a very frail hypothesis, based on actual scarce data, that it would save them from Omicron?
The same could be said about your hypothetical decision to base vaccine passes on 3 shots instead of 2. We know that the 3rd shot offers a marginally better protection against hospitalisation than the first 2 for young adults: studies show a further absolute risk reduction of 1-2% (from 95% to 97%) in the age category <50 y.o (and we only have a meaningful effect on this parameter for people 80+). As said earlier, we know the booster is very inefficient at preventing transmission except maybe for the first 4 weeks after the injection. So, for the vast majority of adults, at least those younger than 70-80, booster shot barely reduces their own individual risk of hospitalisation, does not do much in terms of transmission reduction and, for young males 18-40, seems to carry a higher risk of myocarditis than the COVID-19 infection itself. At the light of this data, you do not have enough arguments to support individual freedom restrictions based on the 3rd dose or not. This 3rd dose, considering how little benefit it has on young adults, should be the result of a free decision not forced upon people.
Please note that my opinion on the 1st and 2nd doses is not the same as for the 3rd dose. Also please note that this opinion would be revised if we had another variant than Omicron emerging.
The situation is different for those 70+ and even more 80+ years old, they definitely benefit from the booster shot and this is the age category where it probably should be mandatory in some way. Because these are the ones dying from COVID-19 in the vast majority of cases worldwide.
Definitely, what COVID-19 should have been is the epiphany of 'personalized public health', i.e. having different public health advice, recommendations and measures based on different population categories, because we have now the capacity to produce this level of finesse. On the contrary, it has been the reign of brutal mass-public policies that can only trigger, in the long run, even more hesitancy towards public health decisions. Public health deciders have to stop taking the common mass of people for fools. People know how to document themselves to a certain extent. And the more you push on them measures and mandates with little to no solid evidence, the more you deter them from accepting the other measures and mandates with solid evidence, because they reject the public health system as a whole. Fool me once, fool me twice…
This is exactly why you shouldn’t in charge of the pandemic response.
The government has given in on the restrictions simply because most people have been ignoring them for some time now. All they did was acknowledge reality. People want to get on with their lives. Whilst I understand your sole focus is the preservation of life, that too comes at a cost.
Meanwhile as a doctor you should be far more concerned about all the other conditions that people suffer from whose testing and treatment have been ignored for the last two years thanks to the focus on the pandemic. My elderly neighbour has been complaining of stomach pains. It could be due to a dozen or more things, some of which are fatal, but the nearest he can get to a doctor is over a phone line.
Andrew: “…as a doctor…”
He isn’t a doctor. This is very likely to be a big part of the problems with this article.
Quite right.
What about those that don’t get treatment in our country and those that get half pie lip service treatment can any of yo on this site relate to that nah! probably not .
Fear of losing the next election has taken over the thoughts of this government and it’s decision making. With a health minister that is completely out of touch with the work force he has sway over little inovation will take place.
With schools I would suggest teachers have a full face screen rather than a mask so the pupils can see the full facial expressions which are very important in forming bonds .
“One was that if something made good clinical sense it would also make good financial sense.”
Not if you’re a psychopathic neoliberal with the smell of public money in your nostrils.
To them, what makes great sense is to lobby dodgy politicians who are similarly inclined to tweak legislation to allow, and indeed encourage, the whole sale theft of public funds to line their pockets while those to whom the money was intended are blamed for being bottom feeding, rivers of filth.
That’s being ‘positive and ambitious, aspirational and confident’ to them while to us we wait for hospital beds with age and worked related injuries and illnesses.
The problem with most good AO/NZ’ers is that they have difficulties grasping the length and breadth of the scale of the swindles now installed into our politic. The swindles span more than 100 years, involve a small and easily manipulated population of trusting souls and stand back agog at just how they get swindled while they remain seemingly powerless to intervene.
AO/NZ doesn’t need a politician. They’re fucking useless. We need an actor. An A lister to come here and act to a script we can write collectively to enable in us a means of address for what the swindlers do to us daily.
We could send in our concerns and ideas and the actor could express them in a manner that might inspire action.
Struggling, under funded public health during a dangerous pandemic while foreign owned bankers steal $6 billion a year in NET profits from us should be a green light for rage and riots. Not whimpering hand wringing.
Thanks Ian. All sound advice (which the Government will ignore), and several very useful links. It looks very much that the Government capitulated to the three-week occupation of parliament grounds in February-March, regardless of its protestations to the contrary. (And the nutters still hard at it in the comments above, I see.)
Sorry Dr Powell.
But you highlight the term.
When all you have is a hammer, every problem is a nail.
You are looking at the problem. From an Elite person with some medical experience(however it would more appear you have trade Union experience as per your previous position.)
The biggest question which is asked about Public health is surely. What is the best thing the Government can do to maximize Public Health.
The NZ Government “”followed the herd”” with lockdowns and alarmism.
While I agree the first lockdown was a reasonable response, given the lack of knowledge about what was happening quickly across the world.
The Zero Covid approach was hilarious NOT supported by many health experts across the world.
IT was suggested by many Non Jacindanistas that it would be reasonable to rampup construction of Hospitals and hospital staff.
But what did this Governmnet do. Extended lockdowns that halted any and all construction,
AND closed the borders to any overseas medical staff that were sorely needed.
The stupidly long Auckland lockdowns stopped many PUBLIC from accessing the health care they needed during that very long period.
I am sorry but your ant is a view thru a keyhole
Good luck with your retirement
Ra, are you a hori tory. Jacinda and the scientists have made the right decisions from the start of the pandemic and that is why she has protected and saved the lives of tens of thousands of Aotearoan citizens from the enemy Covid. You said overseas epidemiologists didn’t support NZ’s strategy – thats why they their governments were failures and ended up with hundreds of thousands of deaths of their citizens. Luckily the useless tories Luxon and Seymore were NOT leading the covid response otherwise they would be losers and failures like the afore-mentioned.
“Hori tory” is an ugly expression Nikorama.
I have given up over comments not being aired on here and I only look in once a week now. It’s taboo to mention cogov/bbbbb.
TDB is becoming an echo chamber…amber…amber.
What’s the matter Magit? Too many right-wingers being called out about their place on the right-wing continuum, from ACT, to Groundswell, BFD, Alt-Right Racists, to Nuremburg, Action Zealandia and Phillip Arps and his mates, to Trump’s White Power Neo Nazis and QAnon.
It’s a Rocky Right Horror Picture Show
If it is a right-wing issue you are complaining about, the problem with WWG1WGA, is that even a little bit to the right on co-governance, is a jump-to the right to Groundswell, another jump to the right to Nuremberg and BFD. Tough job being a right-whingers these days Magit.
A few crocodile tears rolling down my cheeks for you Magit. I can recommend a few counsellors here in Tamaki Makaura for you.
The major logical flaw is that once you have an endemic respiratory virus, you can’t prevent the total number of cases, you can only spread them over time. The fact that a given person will have the virus is almost mathematically inevitable, and in actual fact they are better off getting it now with a relatively fresh vaccine/booster. Unless you commit to a policy of mass vaccination every 3-6 months ad infinitum there will be a proportion of the population with waning immunity even if they’ve followed all the rules.
Hard suppression via extraordinary measures like vaccine passes etc only makes sense when cases threaten to overwhelm the health system in the short term.
The article is really just rank zealotry.